'Surgical' in this context does not mean this technique is to be performed only by a surgeon. Rather the term 'surgical' refers to the fact that some tissue dissection is required with this approach to get from skin to the CTM.
The technique described here uses this kit with a cuffed 5.0 Melker cricothyrotomy cannula. Alternative equipment is available (Patel & Frek, 2008) but the basic principles and steps of the 'surgical' technique are the same:
- Vertical skin incision
- Tissue dissection towards the CTM
- Horizontal incision of the CTM
- (Optional retraction of thyroid or cricoid cartilage with tracheal hook)
- Insertion of a large-bore cricothyrotomy cannula
In more detail, this is the suggested workflow:
1. Position the patient
Head and neck should be extended or even hyper-extended to reveal as much of the anterior neck as possible. In practice this means removing any support/ pillow from under the head.
2. Position yourself
If you are right-handed, stand at the patient's left schoulder. If you are left-handed, vice versa. The non-dominant hand palpates the anatomy and identifies the cricothyroid membrane, the dominant hand dissects and cannulates.
3. Open the kit
4. Identify cricothyroid membrane
Palpate with your non-dominant hand. We suggest to start palpating at the sternal notch with your thumb, index and middle finger, and move upwards along the tracheal rings until the cricoid cartilage is encountered. The 'ditch' above the cricoid cartical is the CTM. Keep your fingers spread slightly to 'fix' the larynx in the midline and keep the CTM between your fingers. This maneuver has been described as the 'laryngeal handshake'. Don't move your hand for steps 5. and 6.
5. Vertical incison over CTM
Make a generous, deep, vertical skin incision of at least 3cm from caudad to cranial over the CTM. Make sure the incision is deep enough to extend all the way down to the laryngeal structures. It could bleed a bit! Keep your palpating hand in place for step 6.
6. Tissue dissection down to CTM and horizontal CTM incision
Tissue dissection down to the CTM can be done bluntly with the index finger of the dominant hand, the Trusseau dilator, or the handle end of the scalpel. Once the CTM itself is identified visually or by palpation, make a generous horizontal incision of the membrane. The CTM has a cartilage border laterally which will stop the scalpel blade straying too far to each side into vascular structures of the lateral neck.
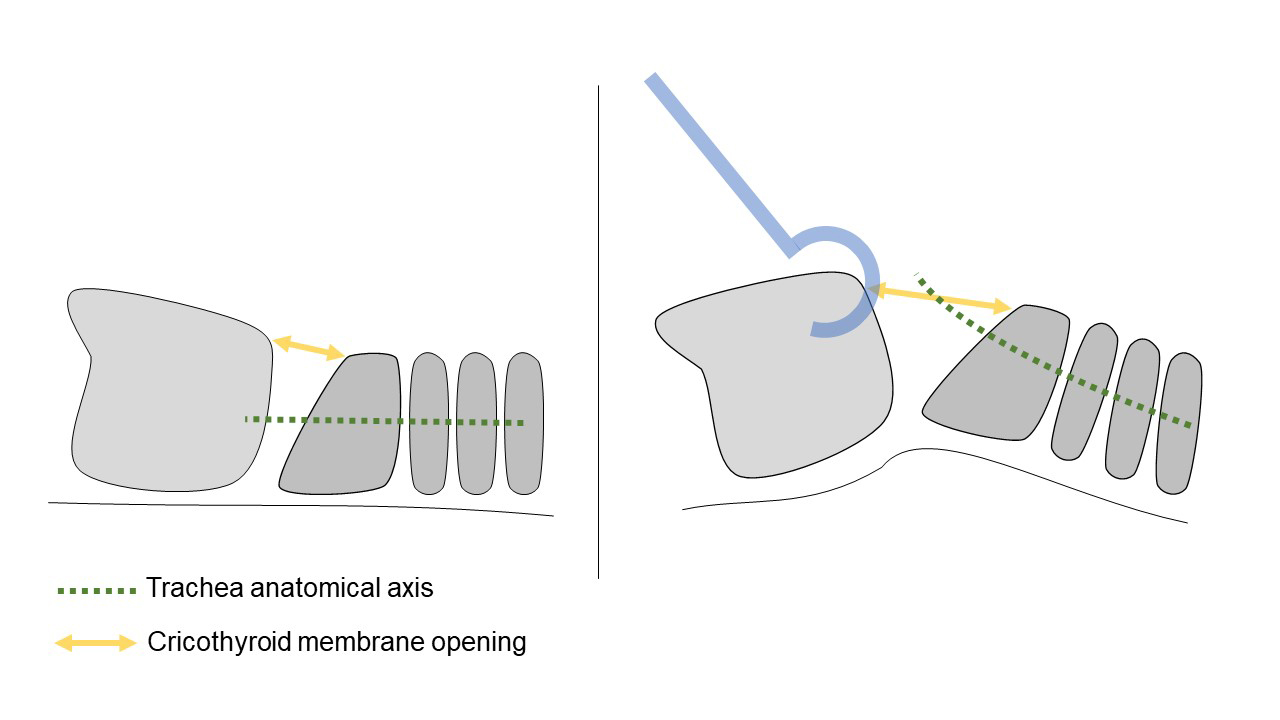
7. Tracheal hook insertion and retraction
The tracheal hook is inserted horizontally through the (also horizontal) incision in the CTM and then rotated 90 degrees so the tip sits underneath the thyroid cartilage. Pull anteriorly and cranially with the tracheal hook to increase the CTM space between the cricoid and thyroid cartilages and bring the axis of the trachea forward for easier cannulation (see below).
8. Advance cricothyrotomy cannula
The Melker cannula is advanced together with the pre-loaded dilator, not sequentially. Grab the cannula so that the dilator does not move/ slide back during advacement through tissue. Note the curvature of the cannula as you insert it in one 'scooping' motion. Do not twist the cannula right and left or 'screw' it into the neck since this is likely to lead to additional trauma and creation of a false passage.
PERSONAL OPINION: The manufacturer of the Melker kit recommends cannula insertion with the Trusseau dilator under 90 degree rotation (see instructional video on the manufacturer's website). This simultaneous rotation maneuver with the Trusseau dilator and the cricothyrotomy cannula is awkward and adds (in my opinion) unnecessary complexity to the technique. It also means you need a second pair of hands to hold the tracheal hook.
9. Remove dilator, secure cannula
Use the included tape around the neck to tie the cannula in place.
10. Oxygenate
The Melker cricothyrotomy cannula has a standard 15mm connector which means you can use any anesthetic breathing system to connect to the device. It is therefore possible to do conventional ventilation and inhaled anesthetic delivery with this technique, like you would through any other 5.0 ET tube.
Add new comment