RAE tubes are named after their inventors Ring, Adair and Elwyn who described the use of their novel oral preformed tube in pediatric patients in 1975 (Ring et al., 1975). RAE tubes were designed with the intention to facilitate intra-oral and some types of facial surgery by keeping the part of the ET tube outside of the patient away from the surgeon's access.
FEATURES
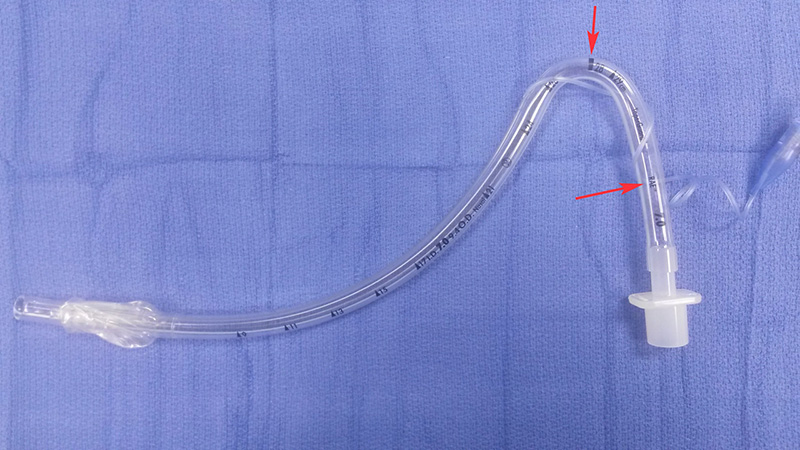
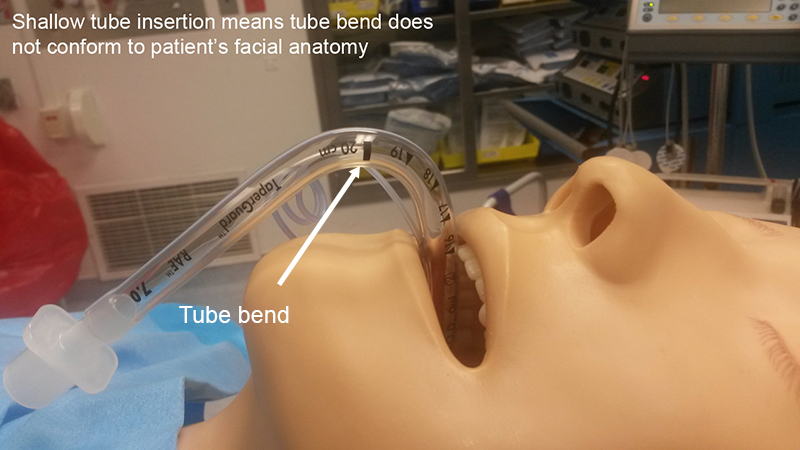
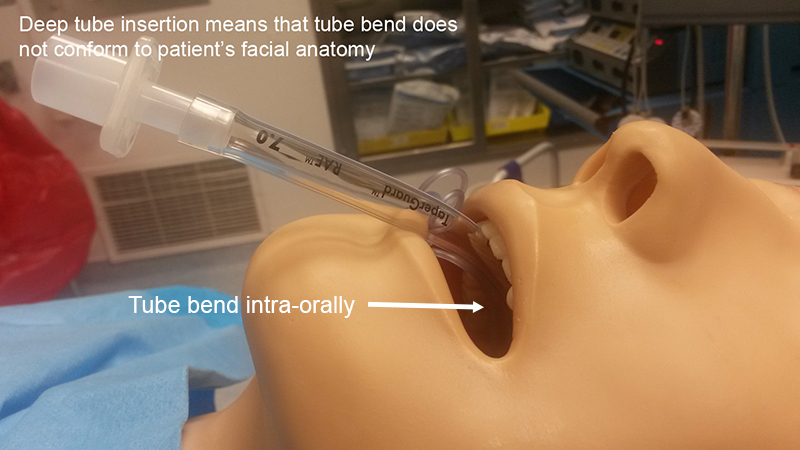
The distinguishing feature of RAE tubes in comparison to 'standard' ET tubes is their different pre-formed bend. The pre-forming during manufacturing reduces the risk of kinking and obstruction which could occur if a 'standard' ET tube was bent into the same shape as a RAE tube. A black marker bar is imprinted on the tube at the point of maximum angle of the bend (see pictures below).
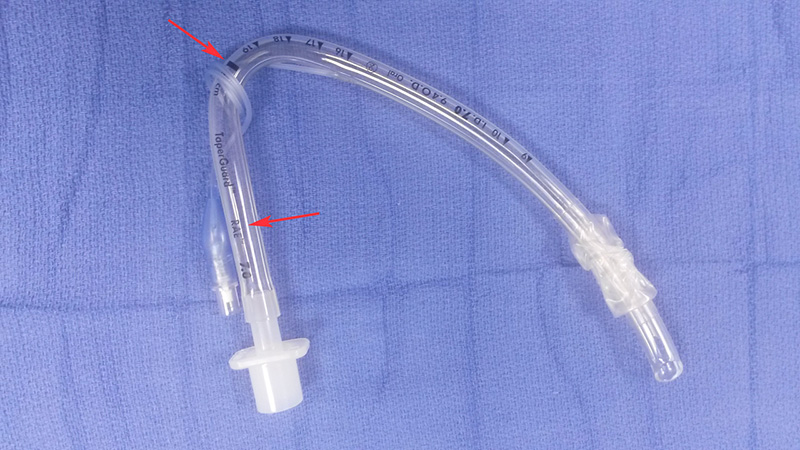
RAE endotracheal tubes are otherwise designed the same way as 'standard' orotracheal tubes, i.e. they have the same left -facing bevelled tip, Murphy eye, cuff design, and length/ diameter markings.
Oral RAE tubes are also described as 'south-facing', i.e. the tube connector facing towards the patient's feet after placement, while nasal RAE tubes are also known as 'north-facing', i.e. the tube connector facing towards the patient's head after placement.
USES
Oral RAE tube
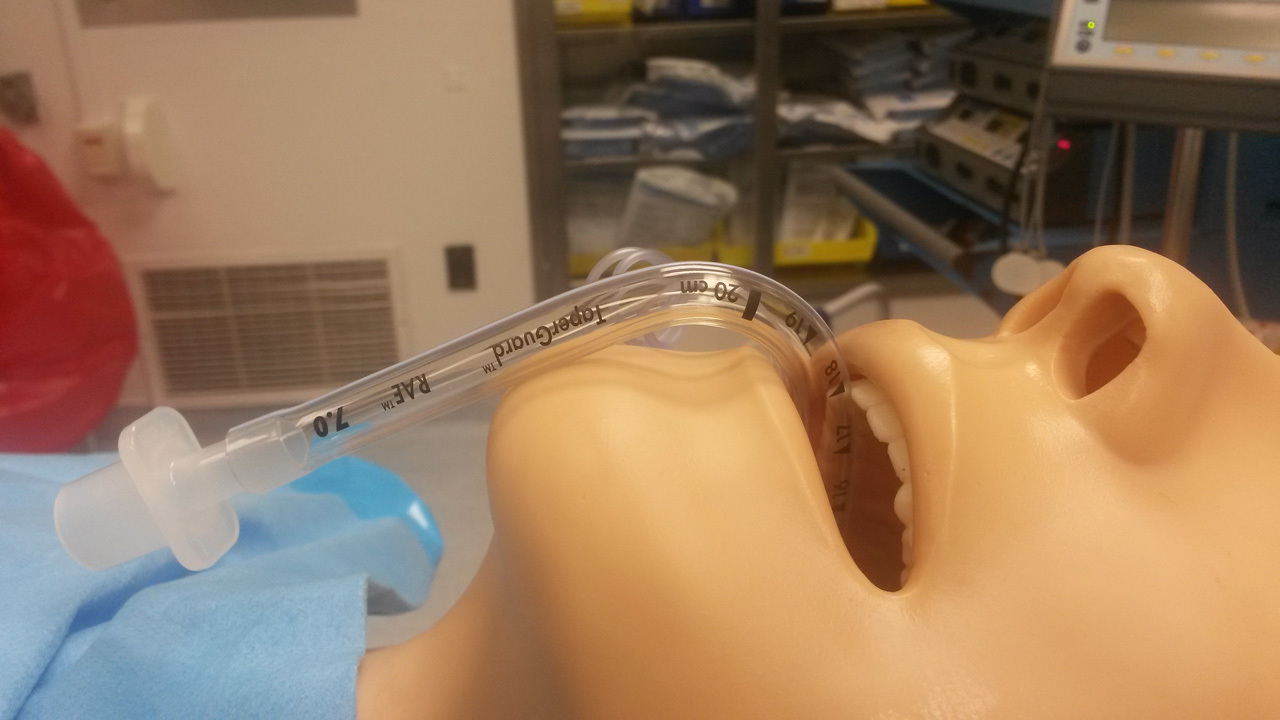
The indications for placing an oral RAE tube are purely surgical, i.e. its use removes the tube connector and anesthetic breathing circuit from the surgical field or access to the surgical field.
Nasal RAE tube
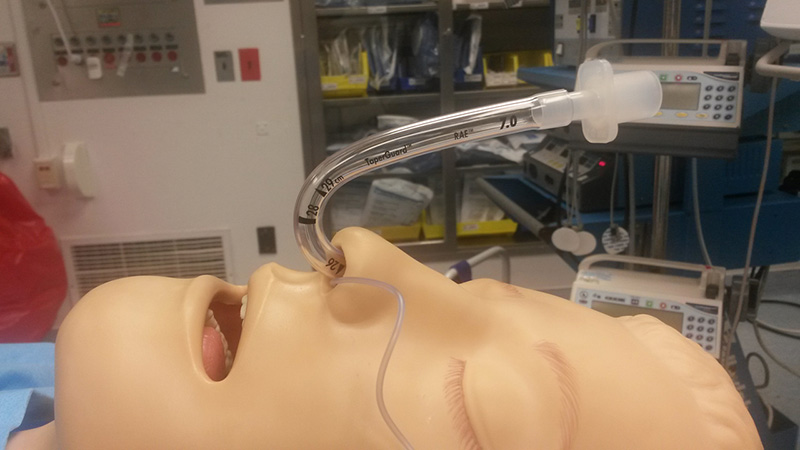
Again, the indications for placing this type of ET tube are mainly surgical as described above. The nasal RAE tube is also the 'go-to' device for many practitioners when performing an (awake) nasal fiberoptic intubation.
SPECIAL CONSIDERATIONS
Disadvantages of the RAE tube
One disadvantage of the nasal (and even more so the oral) RAE tube is that depth of tube insertion is very much pre-determined by the tube's pre-formed shape, i.e. the bend of the oral and nasal RAE will always want to sit just at the lower lip and at the nostril respectively, not allowing you much flexibility as to how deeply you can place the tube into the trachea. In some patients, especially very tall or short ones, it might be difficult to achieve a good tube 'fit' together with the correct insertion depth which avoids accidental bronchial intubation or cuff placement between the vocal chords.
For the oral RAE tube this problem can be avoided by using an armored/ reinforced tube instead. The armored/ reinforced tube can be bent just as much (and more) as the RAE tube without kinking and obstructing.
Securing the RAE tube
Securing the nasal RAE tube is described in the 'Securing the endotracheal tube' section.
The oral RAE tube is best secured by taping it (midline) to the skin between the lower lip and the chin. Use wide tape or a bio-occlusive dressing to get as big a surface area of contact between tube, skin and tape as possible.