Devices in this category are used for oxygen therapy and, in some cases, non-invasive ventilation or respiratory support such as continuous positive airway pressure (CPAP) and non-invasive ventilation (NIV).
Devices delivering high-flow nasal oxygen are dicussed elsewhere
Performance of these devices can be described according to
1. the maximum oxygen concentration achievable to be delivered to the patient,
2. the reliability/ variability with which the devices do that.
Looking at the reliability and variability of oxygen delivery to the patient we can divide these pieces of equipment into fixed performance or variable performance devices. This means that inspired oxygen concentration is either more dependent on the patient's peak inspiratory flow rate (PIFR) (variable performance devices) or less so (fixed performance devices).
Fixed performance devices
These devices deliver a fixed inspired oxygen concentration to the patient, independent of the PIFR. Even at the time of PIFR no random entrainment of room air should occur to unpredictably alter the FiO2 with this equipment.
Devices in this group include:
Venturi masks
There is entrainment of room air with these devices, but it is fixed and not dependent on the patient's PIFR. Therefore the resulting delivered FiO2 is also constant.
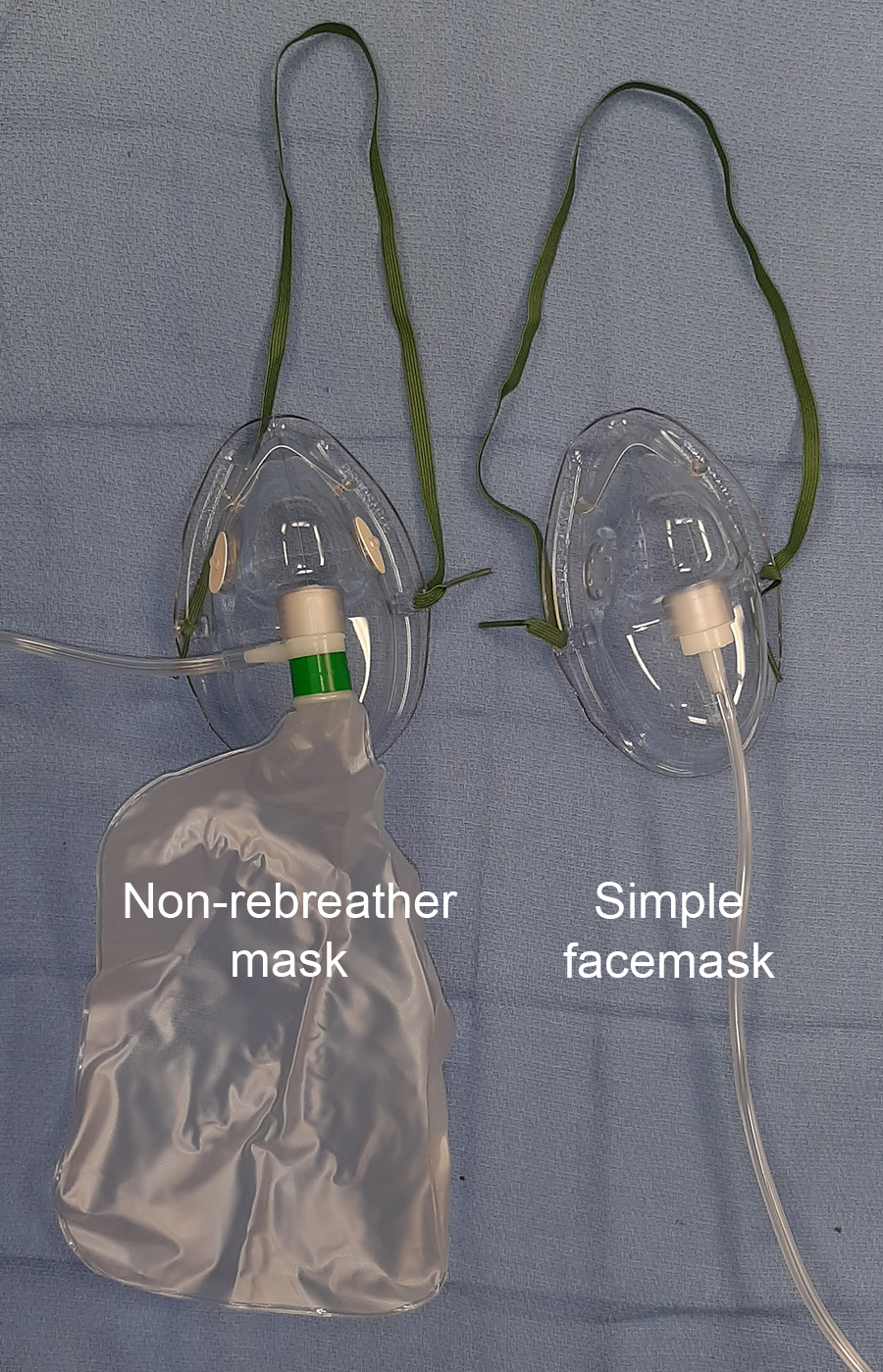
Non-rebreather facemasks
These masks contain a resevoir bag which is connected to the mask with a one-way flap valve, preventing expired gas entering the reservoir. The reservoir bag supplies 100% oxygen and makes up for the deficit in oxygen supply which occurs during times when the patient's PIFR is higher than the oxygen flow to the mask from the wall O2 source.
Non-rebreather mask also incorporate one-way flap valves into the mask itself to prevent indrawing of room air during inspiration.
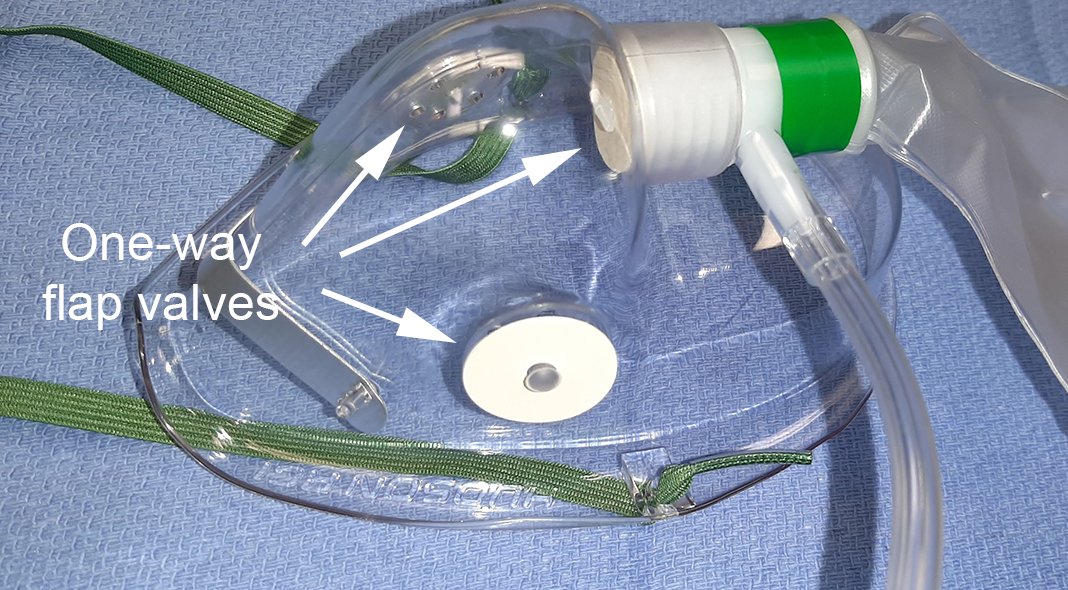
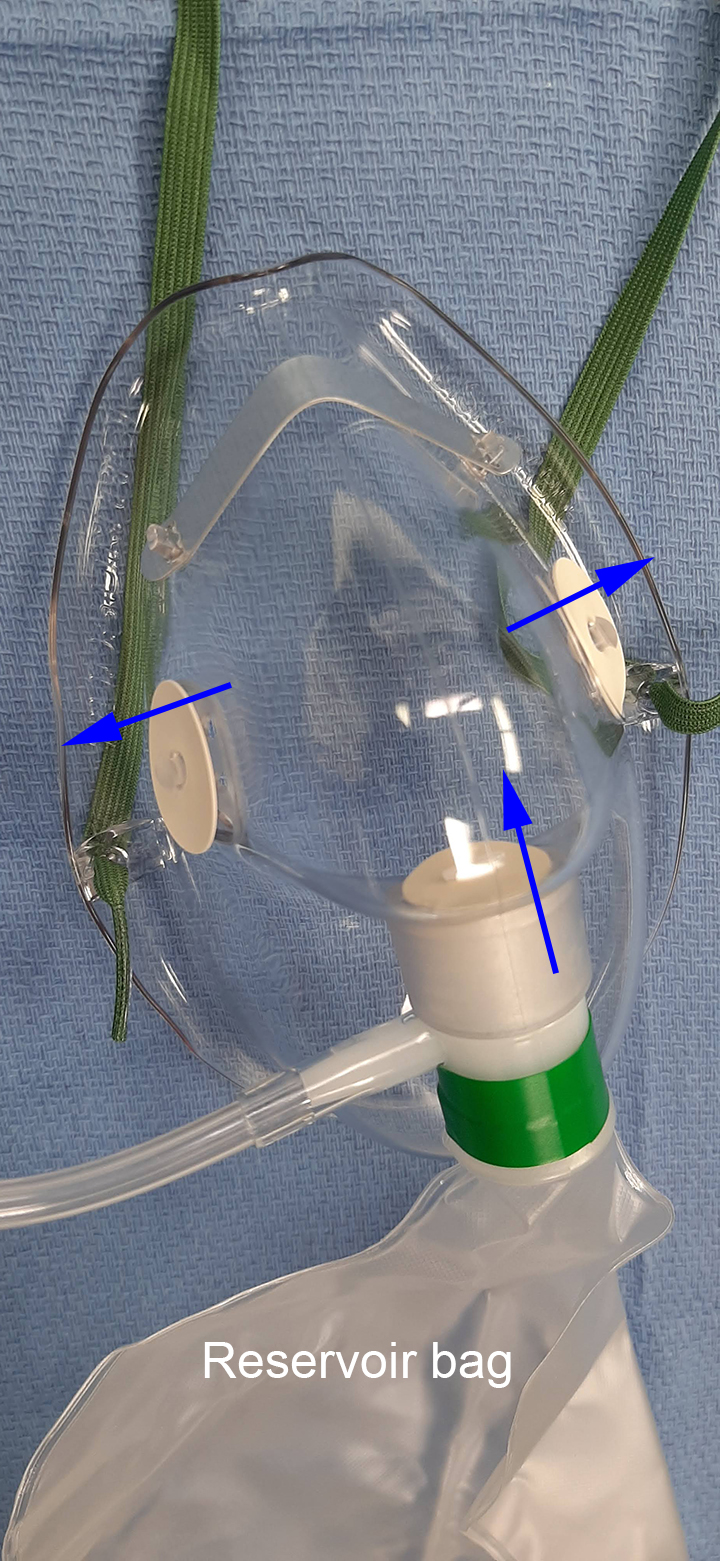
Because of the one-way valves and the reservoir bag these masks should provide a consistent FiO2 (a fixed performance), of up to 60% FiO2 under ideal conditions, such as a good seal between mask and face causing reservoir bag deflation during inspiration, PIFR not too high, etc. In reality, this is often not the case.
Anesthetic facemasks (with a breathing circuit)
These masks form a complete seal around the patient's airway so no entrainment of room air can occur. The delivered oxygen concentration is the same as in the gas mixture supplied to the mask (assuming no rebreathing occurs in the anesthetic breathing circuit).
The Patil-Syracuse and the endoscopy mask also come under this heading. Both of these devices allow instrumentation with a fiberoptic scope or other endoscopic devices while maintaining a seal to the face with the mask.
Variable performance devices
These devices deliver a variable inspired oxygen concentration to the patient, which depends on the PIFR. Depending on a patient's inspiratory effort (tidal volume, 'speed' of inspiration and respiratory rate) the PIFR can often exceed the flow rate at which oxygen or an oxygen/air mixture is supplied by the device, meaning that at the time of PIFR more or less entrainment of room air occurs, altering the resulting FiO2 in an unpredictable fashion.
Devices in this group are:
Nasal cannulas
These range from simple nasal cannulas, ones allowing for monitoring of expired CO2, to high-flow nasal oxygen delivery systems (HFNO systems actually deliver a fixed FiO2).
Simple facemasks/ 'Hudson' masks
These masks, by design, allow entrainment of room air during inspiration through openings in the mask body, which in turn reduces the achievable FiO2.

Comments
nonrebreather masks should
nonrebreather masks should provide FiO2 upto 95% rather 60% under ideal conditions
High Flow nasal prongs are
High Flow nasal prongs are not variable performance. The aspect of low flow cannulae which makes them deliver variable FIO2 is their flow rate in proportion to the minute volume, which can be either very close to MV or almost insignificant compared to it. High flow always delivers much higher flows than MV. Their FiO2 delivery is fixed.
Correct!
Correct!
Add new comment