FEATURES
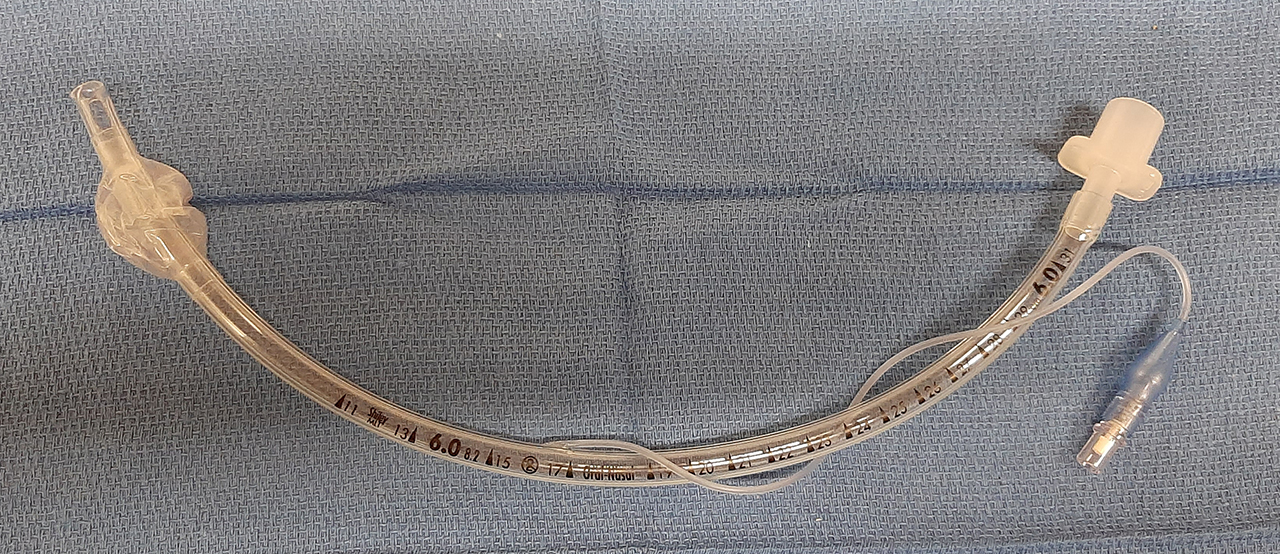
Endotracheal tubes (ETTs) these days are mostly made of polyvinylchloride (PVC) and are single-use. They have a number of characteristic design features that are listed below. Many variations of these designs exist in endotracheal tubes for particular purposes, such as re-inforced tubes, RAE tubes, laser tubes, etc.
Here we just describe the 'standard', most widely used version of an endotracheal tube.
Tube tip design
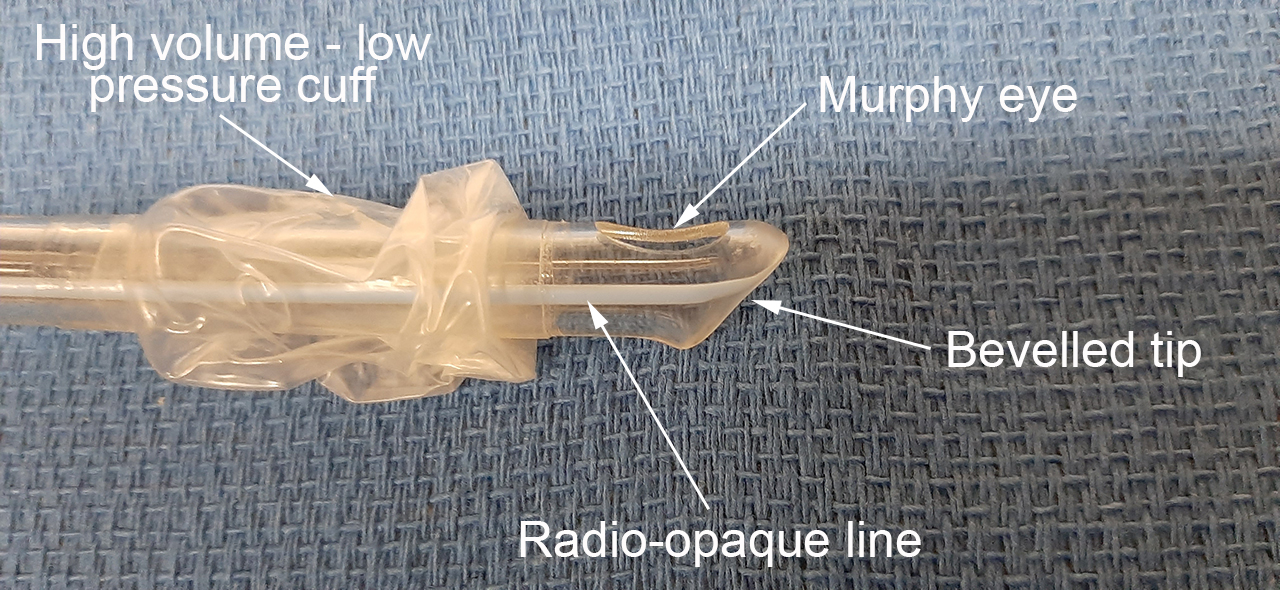
Endotracheal tubes (ETTs) typically have a left-facing bevel at the tip. A bevelled tip will pass much easier through the vocal chords than a a tube with a cross-cut distal opening. The bevel is left-facing rather than right-facing to allow a better view of the ETT tip entering the field of view from right to left/ midline and then passing throught the vocal chords.
Murphy eye
Whilst a tube with a bevelled tip is easier to pass through the vocal chords, it is more likely to occlude when the bevelled opening makes contact with the tracheal wall than a tube with a cross-cut distal opening. The Murphy eye provides an alternate gas passage way should this type of occlusion at the tip occur.
Tracheal cuff
Most endotracheal tubes for use in adults have a tracheal cuff near their distal end. Cuff-less ETTs are also available, and a more commonly used in pediatric patients.
Cuff design
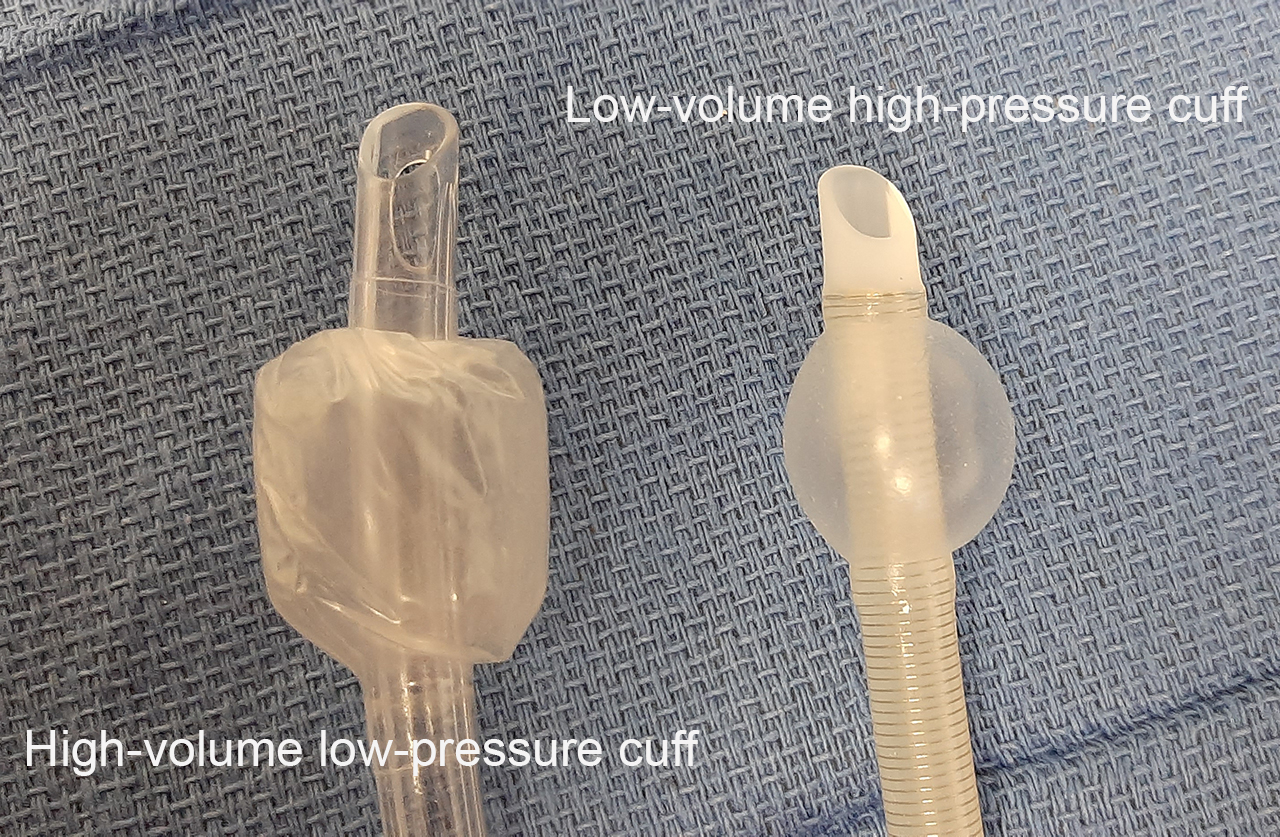
There are generally speaking two types of endotracheal tube cuffs in use, high volume- low pressure cuffs and low volume- high pressure cuffs.
Valve and pilot balloon
The cuff is inflated through a spring-loaded valve with a Luer lock connector. Attached to the valve is a pilot balloon which allows for (rough) tactile and visual confirmation of cuff inflation after intubation or deflation just before extubation.

There is enough clinical evidence availble to proof that 'feeling' the pilot balloon does not give an accurate estimation of cuff inflation, particularly cuff over-inflation which can lead to tracheal mucosal ischemia and subsequent scarring, especially after longer-term intubation. It is therefore important to avoid high cuff pressures and check inflation with a cuff manometer.
Connector
The proximal tip of the ETT has a standard 15mm connector attached to it which allows attachment of a variety of breathing systems and anesthetic circuits. 15mm is the outside diameter of the connector.
Markings on the tube
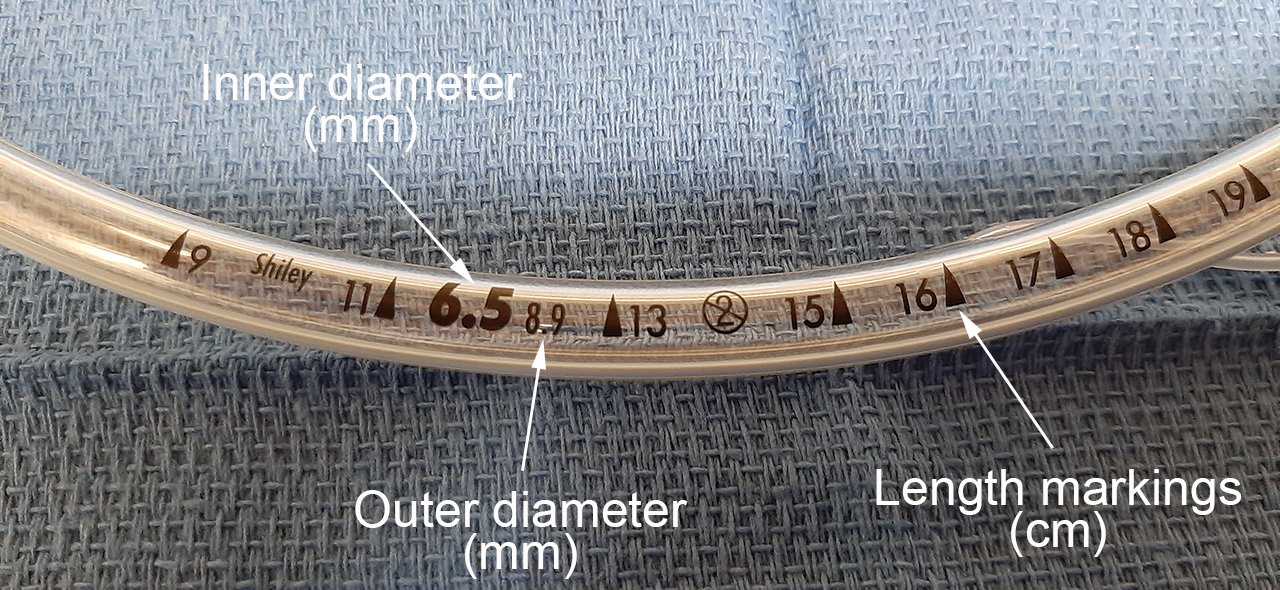
Depending on type and manufacturer ET tubes have several markings on the outside. The ones pretty much all ET tubes have is the size (measured as the inner diameter in mm) and length markings (measured in cm from the tip). In addition, some manufacturers print the outer diameter (in mm) on the tube as well.
Radio-opaque line
Many ET tube include a radio-opaque line which extends all the way to the tip. This is helpful when you want to confirm an adequate tube position on a chest X-ray as the rest of the tube is not going to be visible.
Magill curve
Most ETTs have a pre-formed curve, called the Magill curve, which makes tube insertion easier as the curve follows the anatomy of the upper airway. The 'Magill curve' was a happy accident: When Sir Ivan Magill first used single lumen rubber tubes for nasotracheal intubation in the 1920s, he cut them from a coil of tubing (hence they were curved), and found the curvature useful when inserting these tubes.
The curve should make the use of a stylet unnecessary in most patients.
USES
Endotracheal tube are still considered the 'gold standard' devices for securing and protecting the airway.
Protecting the airway
Airway 'protection' refers to preventing the lower airway, i.e. trachea, bronchial tree and lung, from aspiration. (Cuffed) endotracheal tubes seal the lower airway of at the cuff location in the trachea. Even with a 'good' cuff seal, there is still a risk of micro-aspiration (Hamilton & Grap, 2012), especially with long-term ventilation in the ICU setting.
Again because of the cuff seal, endotracheal tubes allow for positive pressure ventilation without pressure limits within a reasonable physiological range (as opposed to supraglottic airways for example). Endotracheal tubes also facilitate passage of a range of devices into the lungs such as suction catheters, fiberoptic bronchoscopes, bronchial blockers for lung isolation, etc.
REFERENCES
Hamilton, V. Anne; Grap, Mary Jo (2012): The role of the endotracheal tube cuff in microaspiration. In Heart & Lung : The Journal of Critical Care 41 (2), pp. 167–172. DOI: 10.1016/j.hrtlng.2011.09.001.